International Journal of Research Publication and Reviews, Vol 3, no 10, pp 1738-1743, October 2022
International Journal of Research Publication and Reviews
Journal homepage: www.ijrpr.com ISSN 2582-7421
Applications of Robots in Medical Sciences
Krishna Koushik Bhogi
a
, Dr. G. Chandra Sekhar
b
a
B. Tech Student, Department of Electrical and Electronics Engineering, GMR Institute of Technology, Vizianagaram District, A.P, India
b
Professor, Department of Electrical and Electronics Engineering, GMR Institute of Technology, Vizianagaram District, A.P, India.
ABSTRACT
Human research has always been going on in the direction of reducing human intervention in every field to reduce human errors. In Medical field, too, robots have
been in application since the first surgical robot, PUMA 560, was used in 1985 in a stereotaxic operation, in which computed tomography was used to guide the
robot as it inserted a needle into the brain for biopsy. Medical robotics are mainly categorized into 3 types: a) Macro robotics which mainly deal with large size
robots like automated wheelchairs, b) Micro robotics which are mainly used in advanced surgical techniques like Minimally Invasive Surgery (MIS), c) Bio robotics
which mainly deal with simulating biological systems. Telesurgical robotics has appeared as the first area of medical-surgical robotics to reach true global clinical
adoption as a workable solution for robot-assisted minimally invasive surgery (RAMIS). The specific human-in-the-loop control, wherein the skilled surgeon is
always held accountable for the clinical outcome obtained by the robot-actuated invasive equipment, is the reason for its promising performance (still at a low
percentile total market penetration). In this paper, we are going to discuss the several types of robots which are implemented in the medical field till today and the
advancements made in them in some of the major fields in which they are employed, like Robotic Laparoscopy, MRI-guided surgery, Radiosurgery, Soft Robotics,
Minimally Invasive Surgery etc.
Keywords: MIS, RAMIS, Medical Robotics, Laparoscopy, Surgical robot, Soft Robotics, Radiosurgery
1. Introduction
Robotics is one of the most advanced fields today. There are many situations where Robots are used as alternatives for human labour as human intervention
can lead to human errors. And the one field where human errors can be fatal is the medical field. So, there have been many advancements in Robots used
in medical sciences. Many innovative technologies are being developed using medical robots as base such as Minimally Invasive Surgery (MIS), Robotic
laparoscopy, orthopaedics etc. Medical robots are also invaluable players in non-pharmaceutical treatment of disabilities.
In recent years, flexible electronic interfaces and soft robotics have attracted tremendous attention in this field due to their high biocompatibility,
functionality, conformability, and low-cost. The earliest roboticists started investigating the use of robot manipulators for surgical procedures just more
than 30 years ago. Hospitals implemented the first commercial systems twenty years ago. Millions of procedures have been carried out thanks to the
growth of the field of medical robotics over the last ten years, which has resulted in the installation of thousands of robotic surgical systems in hospitals
throughout the globe. Robotics researchers have increasingly concentrated on what the future generation of medical robots might like since it has become
obvious that current healthcare systems embrace surgical robots.
Other aspects of medicine are also being investigated, so their focus is not just on surgical robots. The history of the discipline is thoroughly covered in
the literature, but the original purpose of medical robots was to enable surgeons to operate on their patients remotely and/or with more accuracy. The
early initiatives can be linked to uses in orthopaedic and neurosurgery. Twenty years ago, a transatlantic cholecystectomy was done as the first true long-
distance telesurgery. Although the field's early development was somewhat erratic, as is to be expected with the launch of any completely modern
technology, robot - assisted surgery has matured to the point that the health care sector is now willing to invest significantly in research and development.
2. Literature review
In “A decade retrospective of Medical robotics research from 2010 to 2020”, P. E. Dupont et al., discussed the most advancing technologies in the medical
field in the past decade and the various new Robotic equipment invented. [1]
A platform for cooperative study on developments in surgical robotics is the Raven-II. Seven universities have started using this platform for research.
Dual 3-DOF spherical positioning systems on the Raven-II system allow for the attachment of swappable four-DOF instruments. To make software
development as simple and efficient as possible, the Raven-II program is implemented on open standards like Linux and ROS as discussed by B.
Hannaford et al. [2]
A telerobotics study platform that makes open-source hardware and software available for total access to all control levels was presented by P Kazanzides
et al. The electronics use an FPGA to provide a dispersed I/O and centralised computation architecture, where low-latency I/O is carried out via an IEEE-

International Journal of Research Publication and Reviews, Vol 3, no 10, pp 1738-1743, October 2022 1739
1394a (FireWire) bus at rates up to 400 Mbits/sec while all control calculations are conducted in a familiar development platform (Linux PC). The
mechanical parts are from first-generation da Vinci ® Surgical Systems that have been discontinued. With 11 research institutes now using this system
and more installing it, a research community is being built around a shared open-source platform for hardware and software. [3]
Although the usage of robots has been growing for around 75 years, the medical industry as a whole has only just begun to grasp its potential. This first-
person account traces the growth of robots for the clinical society, the contribution of military medical research, and many of the key initiatives that
helped robotics achieve its present level of accomplishment. [4]
Telerobotic systems' quick development opened the door to new uses outside of the industrial and nuclear fields. Surgeons can now execute medical
procedures from remote locations, away from their patients, thanks to medical telerobotics. Telesurgery solutions facilitate the production of perfect
surgical circumstances and offer a high degree of flexibility and general performance improvement. The initial attempts to create telesurgical devices
adapted the concept from space exploration, where the demand for unique robotics for intrusive treatment even under severe circumstances, like
weightlessness, emerged. Following the same principle, telesurgical devices on Earth first targeted military uses before moving on to civilian ones.
Globally, more than 1.5 million patients receive telerobotic care each year. [8]
Robots have had a significant influence on laparoscopy, neurosurgery, orthopaedic surgery, emergency response, and many other areas of medicine since
they were first utilised in medicine in 1985. This article covers the capabilities of contemporary medical robot systems and offers a history of medical
robots. It largely focuses on commercial products systems while also mentioning a few notable research initiatives. Trends that suggest future capabilities
of surgical robots may be seen by comparing robotic systems across disciplines and time, such as greater intraoperative imaging use, enhanced mechanical
arm design, and tactile feedback to assist the surgeon. [13]
3. Robotic Laparoscopy
When it comes to surgeries, there are a variety of ways to approach it. One method is robotic laparoscopy. With this method, a robot is used during the
procedure. While it is not a popular approach for many surgeons, it is definitely worth looking into if you are going to have a surgery. Surgery can be
scary for patients, so having a robot to perform the surgery alleviates a lot of that fear. The subfield of medical robotics known as laparoscopic robotics
may be the most developed and, undoubtedly, the most lucrative. Three areas have shown advancement in the last ten years: clinical, commercial, and
academic. Clinical research has accounted for an increasingly generous part of laparoscopic robot research. For various surgical procedures, many studies
compare the effectiveness of the robot with conventional (often manual laparoscopic) approaches. Examples include research on hysterectomy, rectal
cancer resection, radical prostatectomy, and radical cystectomy for bladder cancer.
Commercially, the da Vinci robot produced by Intuitive Surgical has continued to evolve over the past ten years [1]. This system features enhancements
to the instrument coupling, the ability to mount endoscopic and laparoscopic instruments on any arm (earlier models had a dedicated endoscope arm),
and semi-automated arm and patient cart positioning. At least 50 new instruments have been made available for the da Vinci over the past ten years.
According to their annual report, the da Vinci has also seen a sharp increase in use, with more than 1.2 million procedures carried out in 2019.
Radical prostatectomy, a radical cystectomy for bladder cancer, the excision of rectal cancer, and hysterectomy are just a few of the procedures that
laparoscopic robots are used for. Robotic versions of manual medical tools such as catheters, bronchoscopes, uteroscopes, and colonoscopes are known
as continuum robots
[2]. In addition to device implantation in the brain and microsurgery within the eye, non-laparoscopic robots have been created for a
variety of uses. Soft sleeves that help the heart contract have been made using soft robotics, and they have also been used to rehabilitate the hands for
daily activities. When a person has mobility limitation or has had a limb amputated, assistive wearable robots are employed to supplement or replace arm
and leg movements.
Fig. 1 - (a) Operating Procedure; (b) Robot Assisted Radical Prostatectomy.
4. MRI-Guided Surgery
Employing medical imaging to direct surgical operations has several documented benefits. A description of numerous such examples was created by a
research consensus panel from the Society of Interventional Radiology. As MRI gives better soft-tissue contrast and spatial resolution, using it to guide
therapies has distinct benefits over using CT and ultrasound for the viewing of soft tissues
[3]. Additionally, MRI offers concurrent imaging of soft tissue
International Journal of Research Publication and Reviews, Vol 3, no 10, pp 1738-1743, October 2022 1740
and interventional tools (such as needles and catheters), allowing for interactive adjustment and control of the interventional strategy. Additionally, MRI
has the ability to sense a wide range of physiological signals, such as oxygenation, flow, temperature, strain, and others as a multiparametric imaging
technique.
The ability to improve accuracy is one of the main advantages of MRI-guided robot-assisted procedures. Because of closed-loop control and well-
coordinated multi-axis motion, robotic aid may increase positioning precision and repeatability. To make sure that the operative plan is carried out as
intended, intraoperative MRI may specifically measure tissue movements and tool deflection.
To dynamically modify intervention tactics, imaging can help with instrument monitoring and motion compensation. As a striking example, Hatiboglu
et al. discovered that in more than 40% of documented glioma surgery instances, the surgeons revised their surgical strategy based on newly acquired
data from intraoperative MRI. Additionally, robot-assisted treatments with MRI guidance can considerably enhance ergonomics. The closed-bore scanner
makes manual interventions difficult and, in some situations, impossible from an ergonomic standpoint. The distance to the isocenter of a conventional
closed-bore MRI scanner is 75–90cm, with a bore diameter of 60–70cm
[4]. Additionally, while extending into the bore, it is challenging to view
intraoperative MRI. Although there have been more low field open scanners developed for surgical interventions, their field strength and picture quality
are inferior to that of an adoption of high field closed-bore diagnostic scanner. Between MRI-guided and fluoroscopy-guided treatments, Fernández-
Gutiérrez et al. examined the ergonomic procedural differences.
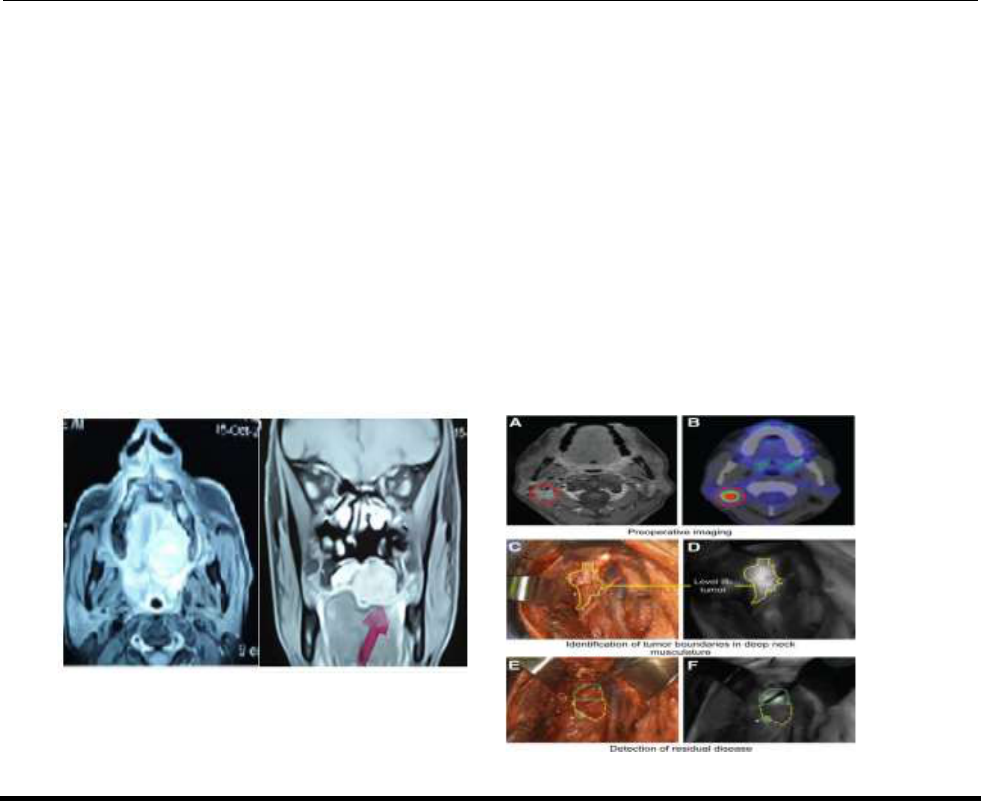
Fig. 2 - (a) Axial & coronal MRI of palatal mass; (b) Disease detection.
5. Radiosurgery
Focused beams of ionizing radiation are aimed at the patient during radiosurgery, a form of therapy (not surgery), largely used to treat malignancies [5].
High-dose radiation is supplied to the tumour while the epithelial layer receives much less radiation by orienting the radiation through the tumour at
different angles. Before real-time tissue monitoring, radiosurgery was essentially restricted to employing stereotactic frames attached to the cranium with
bone screws to treat the brain. Systems are now marketed because actual tissue tracking is practical. The goal of radiosurgery is to treat diseases of the
brain, spine, and nervous system with a high level of precision through the use of focused beams of radiation. This technique is able to focus on small
target areas with minimal damage to surrounding tissues.
A prosthetic arm having a linear accelerator, a six-degree-of-freedom robotic patient table termed the RoboCouch, as well as an X-ray image processor
that can simultaneously capture images in two perpendicular orientations in real time are all components of the frameless radiosurgery system known as
the CyberKnife (Accuray Inc.) [6]. The two concurrent intraoperative X-ray pictures are used to register a high-quality preoperative CT image but are
insufficient to offer a clear description of the tumour. The premeditated radiation dosage can then be administered using a variety of orientations by the
robotic arm. A frameless system with a linear accelerator, the Novalis using TrueBeam STx (BrainLab Inc. and Varian Medical Systems, formerly Novalis
and Trilogy, first FDA certification 2000) uses micro-multileaf collimators for beam shaping
[7].
Intraoperative X-rays are compared to CT scans similarly to CyberKnife, and epidermis fiducials are visually monitored in real-time. Cone beam CT is
also a part of the delivery system. The patient is positioned on top of a robotic sofa with six degrees of freedom. The Cyberknife radiation source offers
more flexibility in how it can be positioned around the patient than the Novalis, which can also shape the beam of radiation and claim a lower out-of-
field dosage.

International Journal of Research Publication and Reviews, Vol 3, no 10, pp 1738-1743, October 2022 1741
Fig. 3 - (a) CyberKnife model; (b) Left Trigeminal Neuralgia scan.
6. Soft Robotics
It is difficult to pinpoint the robotics breakthrough that gave rise to the discipline of soft robotics in medicine. Robotics built on soft principles, naturally
flexible structures, and intelligent materials have always been intricately linked to biomimetics and bioinspiration. The research on intelligent materials
that may be used to fabricate soft robots or to give soft robots actuation and sensing abilities, from the macro-scale through to the nanoscale, has been
prompted by the rising interest in bioinspired robots with flexible bodies
[8]. Even though it has not yet created paradigmatic instances of medical robotic
systems, the discipline of soft robotics is guiding the research and development of the majority of medical instruments. Parallel to this, research in soft
substances and cutting-edge manufacturing techniques is being encouraged by soft robotics, which may lead to unanticipated developments in biomedical
applications.
As an illustration, the majority of research on prosthetic skins with sensing devices has been done for soft robots and other soft devices. If one looks at
the literature from the past ten years
[1]
, there are a lot of fundamental reviews and surveys on soft and bioinspired robotics for many applications (including
medicine, in which the issue of intrinsic safety is highly relevant), as well as a lot of papers and reviews on innovative smart materials where conventional
silicon-based technologies for detection are supplanted by silicone-based innovations with smart behaviour. Excluding materials articles and survey
papers from the last ten years' most-cited papers, two categories of medical works may be distinguished: One consists of portable soft robots for human
enhancement or rehabilitation, which have been discussed in earlier sections.
The second category consists of surgical and interventional robots as well as their component parts. Three parallel subtopics may be found in surgery and
intervention: Soft, bioinspired, or responsive components, which can function as standalone devices or could be incorporated into more conventional
systems, including soft devices for treatment or intervention, in which the entire conventional equipment is substituted by a soft robotic layout, at both
the macro and micro scale
[9]
. For surgery and endoscopy, various intriguing designs of modular devices with variable stiffness have been created and
advanced to the preclinical or cadaver test stage. By simply varying the rigidity of the various parts, surgical manipulators may be transformed into
octopus' arms or elephant trunks with the potential to do multiple jobs with a single arm. With the invention of soft-body capsules for conducting targeted
medication administration, as already shown, relevant findings have also been obtained by using soft robotics technology to gastrointestinal capsule
endoscopy.
Fig. 4 - (a) Soft Robot prototype; (b) Movement Range.
7. Minimally Invasive Surgery
Although the precise creator of the concept of tele robotic surgery has not been found, some early pioneers at the U.S. National Aeronautics and Space
Administration (NASA), the U.S. Department of Defense, and the Defense Agency for Advanced Research Projects (DARPA) established the foundations
and the late 1960s saw the beginning of the domain's foundations, influenced by the remote controls used in nuclear power–Facilities and space
development. Because of this, the first FDA-cleared product has achieved tremendous commercial success
[10].
In 2000, it was clear that RAMIS system, an innovative system that numerous further studies and businesses focused on developing custom systems with
minimal to no divergence, named da Vinci was developed. The former was passed by intuitive
[11]
. Computer Motion (Goleta, California, USA), a rival,
in 2003, and their Zeus Robotics Surgical System was discontinued
[10]
. The several types and adaptations of these systems were examined in a recent
International Journal of Research Publication and Reviews, Vol 3, no 10, pp 1738-1743, October 2022 1742
analysis by Moglia et al. The advancement of surgical automation and the incorporation of force sensing into laparoscopic tools, along with novel robot
architectures designed to minimize procedural invasiveness, were among the early efforts that Dupont et al. identified as the most significant
advancements of the previous ten years. The DVRK, an open hardware and software platform developed first by Laboratory for Computational Sensing
and Robotics (LCSR) at Johns Hopkins, Worcester Polytechnic Institute (WPI), and partners with funding from the Intuitive Foundation
(https://www.intuitivefoundation.org/dvrk/), is arguably the most noteworthy recent achievement on the research platform front
[12]
.
The most crucial aspect of a robotic system’s applicability is likely its autonomy. The level of autonomy (LoA) idea, which was first put forth for the
automobile sector, has also begun to be used in medical robotics to help identify and assess system capabilities. It expands on the traditional paradigm of
task analysis along the generate-model-plan-execute cycle, an overarching autonomy notion seen in everything from mechatronics to image-guided
interventional systems. Considering a large control loop frequency, the traditional surgical CAD/CAM control schematic is essentially applicable for
even RAMIS systems. This proves that the core idea that digital information, through diagnostic imaging, image analysis, and robotic execution, allows
accountable, measurable systems design, and quality management ideas in CIS, is entirely true in the case of RAMIS as well.
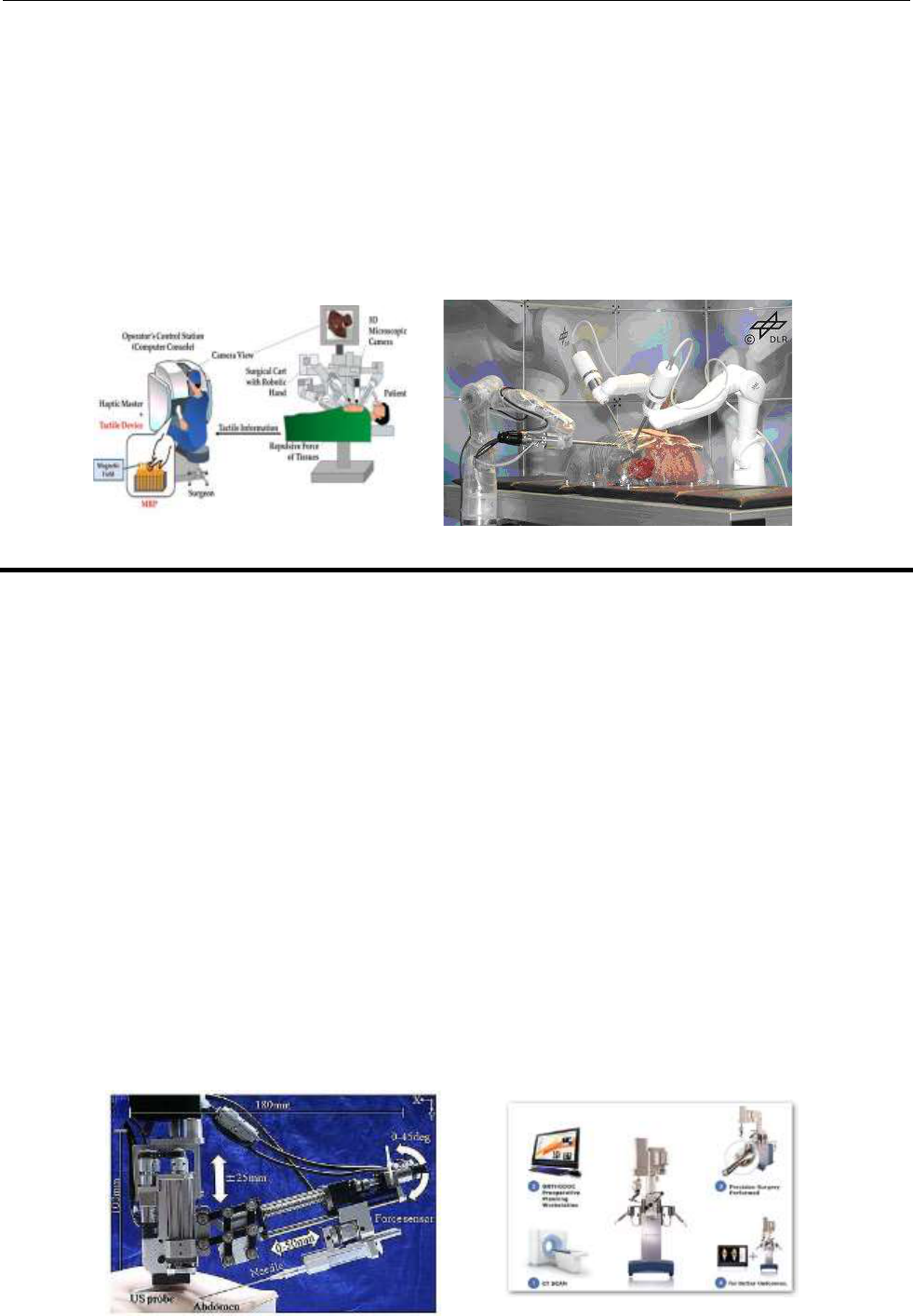
Fig. 5 - (a) RAMIS System; (b) Da Vinci Robot.
8. Orthopedics
Precise and accurate bone excision is the anticipated orthopaedic advantage of robot aid. Robotic technologies can enhance the alignment of the implant
with the bone and expand the contact area between bone and implant through effective bone resection, both of which may enhance functional results and
implant lifetime.
Up to now, orthopaedic robots have focused on replacing or resurfacing the hip and knee (the Renaissance system and its spine usage being the only
known exception). All methods employ bone screws or pins to localize the surgical site, unlike early systems that needed the bones to be set in place.
Robodoc (Curexo Technology Corp., initially by Integrated Surgical Systems), which was utilized for the first time for a complete hip replacement in
1992, provided the first robotic help for orthopaedic surgery. Robodoc has acquired FDA certification for complete hip replacement (1998) as well as a
CE mark (1996)
[13].
The surgeon designs bone milling using OrthoDoc, a surgical planner, and the robot in combination with preoperative CT. The patient's leg is secured to
the robot's pedestal during the surgery, and a secondary clamp identifies the femoral head to cause the robot to stop if the leg moves. The milling is then
automatically carried out by Robodoc in accordance with the surgical plan. Such independent motions were used in many early surgical robotics projects,
raising questions regarding the safety of both patients and medical professionals.
The RIO robotic arm, manufactured by MAKO Surgical Corp and formerly known as the Tactile Guidance System, was introduced and given FDA
approval in 2008
[14]
. In addition to patellofemoral arthroplasty, the RIO is utilized to implant medial and lateral unicondylar knee components. In keeping
with the movement away from autonomous robot actions, the surgeon and the RIO both grip the surgical instrument while they navigate the operative
site. The arm's low friction, as well as low inertia design, makes it simple for the surgeon to maneuver the tool, back-driving the joint actuators in the
process. The arm's role throughout the milling process is to serve as a haptic device, opposing actions outside the intended cutting envelope by gently
forcing on the surgeon's hand. Unlike other orthopedic systems, the RIO relies on a video system to watch bone pins and instruments intraoperatively and
instantly register the anticipated operating area to the patient in the operating theatre. This is in contrast to other orthopedic systems that need the bone to
be secured in place. The technology shows potential as a surgical teaching instrument in this form.
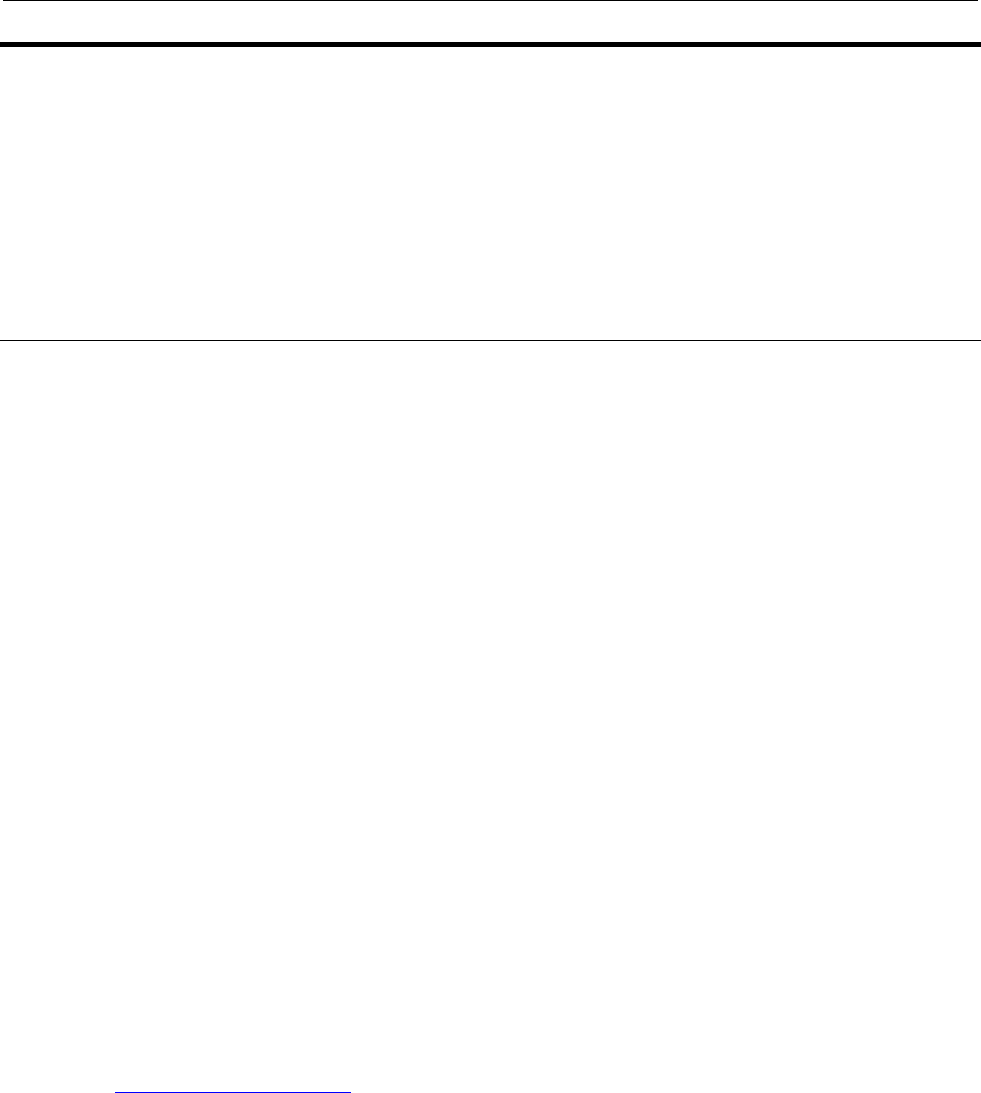
Fig. 5 - (a) OrthoDoc; (b) Applications of OrthoDoc.
International Journal of Research Publication and Reviews, Vol 3, no 10, pp 1738-1743, October 2022 1743
9. Conclusion
Robotics in the medical field have gone far past the testing stage and are in use all over the globe for various applications. Even now, due to the COVID-
19 pandemic, many hospitals are more inclined to employ robotic devices in a wide range of tasks to reduce the exposure to pathogens as much as
possible. They are also helping in limiting human contact. But the key issues in medical robotics right now are automation and autonomous decision-
making.
As much as human research has progressed, complete automation is still not possible for medical robots, so there is always a supervisor needed. Also,
due to the lack of autonomous decision-making, medical robots lack the adaptability needed in the medical field due to the many types of variations one
can observe in every case, once again needing supervision.
These are the present issues being faced and the current research directions in the field of medical robotics.
References
[1] P. E. Dupont et al., “A decade retrospective of Medical robotics research from 2010 to 2020,” Sci. Robot., vol. 6, no. 60, Nov. 2021, Art. No.
eabi8017.
[2] B. Hannaford, J. Rosen, D. W. Friedman, H. King, P. Roan, L. Cheng, D. Glozman, J. Ma, S. N. Kosari, L. White, Raven-II: “An open
platform for surgical robotics research.” IEEE Trans. Biomed. Eng. 60, 954–959 (2013).
[3] P. Kazanzides, Z. Chen, A. Deguet, G. S. Fischer, R. H. Taylor, S. P. DiMaio, “An open-source research kit for the da Vinci® Surgical
System”, in Proceedings of the 2014 IEEE international conference on robotics and automation (ICRA), Hong Kong, China, 31 May to 7 June
2014.
[4] R. M. Satava, “Surgical robotics: The early chronicles: A personal historical perspective,” Surgical Laparoscopy, Endoscopy Percutaneous
Techn., vol. 12, no. 1, pp. 6–16, Feb. 2002.
[5] R. Schulz and N. Agazaryan, “Shaped-Beam Radiosurgery: State of the Art”, Springer, New York, NY, USA, 2011.
[6] J. R. Adler Jr., S. D. Chang, M. J. Murphy, J. Doty, P. Geis, and L. Hancock, “The cyberknife: a frameless robotic system for radiosurgery,”
Stereotactic and Functional Neurosurgery, vol. 69, no. 1–4, pp. 124–128, 1997.
[7] G. J. Gagnon, N. M. Nasr, J. J. Liao et al., “Treatment of spinal tumors using cyberKnife fractionated stereotactic radiosurgery: pain and
quality-of-life assessment after treatment in 200 patients,” Neurosurgery, vol. 64, no. 2, pp. 297– 306, 2009.
[8] A. Takács, D. A. Nagy, I. Rudas, and T. Haidegger, “Origins of surgical robotics: From space to the operating room,” Acta Polytechnica
Hungarica, Vol. 13, no. 1, pp. 13–30, 2016.
[9] T. Ginoya, Y. Maddahi, and K. Zareinia, “A historical review of medical robotic platforms,” J. Robot., vol. 2021, pp. 1–13, Jan. 2021, Doi:
10.1155/2021/6640031.
[10] T. Haidegger, S. Speidel, D. Stoyanov and R. M. Satava, "Robot-Assisted Minimally Invasive Surgery—Surgical Robotics in the Data Age,"
in Proceedings of the IEEE, vol. 110, no. 7, pp. 835-846, July 2022, Doi: 10.1109/JPROC.2022.3180350.
[11] J. Klodmann et al., “An introduction to robotically assisted surgical systems: Current developments and focus areas of research,” Current
Robot. Rep., Vol. 2, no. 3, pp. 321–332, Sep. 2021, Doi: 10.1007/s43154-021-00064-3.
[12] A. Race and S. Horgan, “Overview of current robotic technology,” in Innovative Endoscopic and Surgical Technology in the GI Tract. Cham,
Switzerland: Springer, 2021, pp. 1–17, Doi: 10.1007/978-3-030-78217-7.
[13] Ryan A. Beasley, "Medical Robots: Current Systems and Research Directions", Journal of Robotics, vol. 2012, Article ID 401613, 14 pages,
2012. https://doi.org/10.1155/2012/401613
[14] J. Rosen, B. Hannaford, and R. Satava, Eds., “Surgical Robotics: Systems Applications and Visions”, Springer, New York, NY, USA, 2011.
