Response-based sleep intervention: Helping infants sleep without
making them cry
☆
Wendy Middlemiss
a,
⁎
, Helen Stevens
b
, Lael Ridgway
c
, Susan McDonald
c,d
, Michelle Koussa
a
a
Department of Educational Psychology, University of North Texas, Denton, TX, United States
b
Parent Infant Consultants, Melbourne, Australia
c
School of Nursing and Midwifery, La Trobe University, Melbourne, Australia
d
Mercy Hospital for Women, Melbourne, Australia
article info
Article history:
Received 6 December 2016
Received in revised form 16 March 2017
Accepted 21 March 2017
Available online xxxx
© 2017 Elsevier B.V. All rights reserved.
1. Introduction
It is common for parents to raise questions about infant sleep pat-
terns when attending infant well-visits during the first year of life [1,
2]. In seeking answers to their questions from health practitioners,
parents have access to a myriad of resources, including family, friends,
web-based sites, social media , as well as parenting books. However,
these sources of information often present contradictory best practice
recommendations [3]. These contradictions are particularly notable in
the areas of Infant Total Sleep time (TST) and parental response and
presence when infants transition to sleep [4,5]. With the frequency of
parents' ques tions about infant sleep, helping parents to establish
healthy sleep patterns during an infant's firstyearoflifeisanimportant
concern for researchers and practitioners. At present, between 25% and
40% of families report childhood sleep problems defined by latency to
sleep, number of infant night wakings, and inability to return to sleep
without parental attention [6,7,8]. Infant night wakings accompanied
by infant signaling for attention (e.g., crying) are identified as problem-
atic for parents due to disruptions in sleep, parental fatigue [9] and an
association between wakings and maternal depression [10,11].
Given an association between parent presence and infant signaling
during nighttime care, recommendations often caution parents against
responding to infants during their transition to sleep or when waking
[12]. Based on this goal, most commonly recommended best practices
focus on limiting parental presence and response to infant signals for
attention during transitions to sleep. These practices include unmodi-
fied extinction approaches, such as crying it out or unmodified extinc-
tion characterized by parental nonresponse to infant crying [12,13];
modified or gradual extinction-based approaches, such as controlled
comforting characterized by continued decrease in parental response
and presence when infants transition to sleep [12,13]; or fading rou-
tines, such as camping out or scheduled wakings [12,13]. With adher-
ence to b ehavio ral protocols, each of th ese practices is shown to be
effective in training infants to transition to sleep without parental inter-
action [14,4].
Despite their success, a signifi cant body of research suggests that
these recommended behavioral practices may have some drawbacks
for both parents and infants. For example, parents have been reported
to experience discomfort with leaving an infant to cry to sleep or in lim-
iting presence during transitions [15,13]. Whether parental responsive-
ness when infants transition to sleep is helpful or hindering for infant
emotional development remains an area of controversy [16].Similarly,
the role of responsiveness for infants' developing regulatory systems is
debated [17,18,19,20,21]. Finally, questions of whether parent and
infant sleep quality is benefited or hindered by parent presence remain
unclear [22].
These debates in the research are evidenced in the limited assess-
ment of behavioral sleep approach es. Limiting parent presence as a
mechanism to reduce night wakings is supported by the work of Price
and colleagues who examined children's development following the
use of modified behavio ral approac hes with infants identified with
sleep problems at 7 months of age. Their longitudinal study identifi
ed
no
negative impact in the group of mothers engaged in this behavioral
Early Human Development 108 (2017) 49–57
☆
Grant information: This research was funded through a 2014 Victorian State
Government Department of Economic Development, Jobs, Tr ansport and Resources,
Grant to Safe Sleep Space Pty. Ltd. (Innovation Voucher Program Research and
Development Voucher (IVP BDR) 123 A,B,C) via La Trobe University.
⁎ Corresponding author at: Department of Educational Psychology, University of North
Texas, 1155 Union Circle, #311335, Denton, TX 76203, United States.
E-mail address: wendy.middlemiss@unt.edu (W. Middlemiss).
http://dx.doi.org/10.1016/j.earlhumdev.2017.03.008
0378-3782/© 2017 Elsevier B.V. All rights reserved.
Contents lists available at ScienceDirect
Early Human Development
journal homepage: www.elsevier.com/locate/earlhumdev
sleep program [14]. Mothers engaging in the sleep program were en-
couraged also to engage in authoritative parenting practices with their
child [23]. Given that authori tative parenting practices h ave been
strongly linked to healthy child outcomes [24], the presence of this rec-
ommendation in the program makes it unclear whether child outcomes
are related to earlier sleep routines.
In a study examining mother and infant cortisol levels during a sleep
training program, participation was associated with cessation of infant
crying when transitioning to sleep—supporting the successfulness of
this approach to extinguishing infant signaling. Associated with this ces-
sation of crying was a decrease in maternal cortisol levels. However,
there was not a corollary decrease in infants' cortisol levels across the
residential program [25]. As this research did not examine cortisol levels
around sleep following program completion, the long-term implica-
tions of these findings are not known.
1.1. Focusing on responsiveness
To add ress questions about infant sleep patterns, parent support,
care presence, and behavioral modification approaches to increase in-
fant TST and crying, this research examines the role of responsiveness
to infants during their transitions to sleep. This research explores
whether a response-based sl eep intervention increases infant TST
without limiting parent presence or use of a behavioral sleep program
focused on extinguishing infant crying during sleep.
Overall, responsiveness to infant signals has been established as im-
porta nt to their development and well-being [26,27,28].Thisisevi-
denced in research examinin g the role of emotional responsivity in
infant development. Emotional responsivity, which entails expressing
as well as responding to emotional signals of another individual, has
been identified as crucial to the attachment relationship [29] and, ulti-
mately, important in the development of a child's autonomy. Feldman
[17] discussed the concept of synchrony, a related concept which refers
to the biologically driven rhythmic nature of the parental response to
infant signals and infant response to parental care. Through continuing
action and response, the parent-infant pair develops a relationship that
assists the growing child in developing self-regulation and positive
social relationships [30].
A lack of response to infant cries at night or being inconsistent in
responding between day and night signals for care may lead to in-
creased infant stress [31] with caregiver responsiveness necessary to
help infants self-regulate their physical and emotional responses to
stress [28]. This view is supported by research in which there was an in-
crease in autonomic system arousal in neonates during episodes of ma-
ternal separation [32]. These researchers suggested that the infant who
received more attention at n ight may have more exte rnal emotional
regulation assistance than those who sleep alone at night and do not re-
ceive as much nocturnal attention [32]. This would suggest that infant
emotional needs continue through the night and responding to infant
signaling encourages the development of self-regulation by infants.
In research examining infant sleep and mothers' emotional availabil-
ity, Teti and colleag ues [33] forward emotional availa bility as an
important part of bedtime practices. Specifically, mothers' emotional
availability was related to fewer infant night wakings and fewer times
mothers had to re turn to their infants at bedtime [33].Mothers'
emotional availability was inversely related to their rating of whether
infants had sleep difficulties [33].
A number of reviews have considered the relationship between ma-
ternal mood and infant sleep [10,34]. For example, changes in maternal
sleep physiology and related fatigue can contribute to maternal depres-
sion during the postpartum period
[10,34].
As the symptoms associated
with depression may impact the perceived emotional availability of the
mother, the maternal responsiveness observed to help alleviate infant
sleep disruptions may not be as prevalent. Though an association has
been observed between the depressive symptomatology of the mother
and infant sleep, the causations of maternal depression and infant sleep
behaviors have not been clearly identified to what is a causative factor
and what is a resulting factor in infant sleep disturbances [10,35].
1.2. Current study
This research provides the first empirical examination of the effec-
tiveness of a non-behaviorally based sleep intervention in increasing in-
fant TST through mother-infant participation in a response-based sleep
program. By examining both infant TST and maternal and infant physi-
ological markers of stress during a sleep intervention, this research will
be helpful in informing current debates regarding infant sleep practices
and parent responsiveness.
1.3. Hypotheses
1.3.1. Mothers' and infants' participation in a response-based, resi-
dential sleep intervention will increase infant TST from Pre-Admission
to Days 1, 2, and 3 of the program intervention and nine days after
program completion.
1.3.2. Infant TST will increase from Pre-Admission to Days 1, 2, and 3
of the program intervention and nine days after program completion for
mothers reporting significant levels of depression, anxiety, or stress.
1.3.3. Participation in the response-based residential sleep interven-
tion will be associated with decreases in infant and maternal cortisol
levels from Pre-Admission to nine days after program completion.
2. Methods
2.1. Study context
Changes in infant TST and maternal and infant levels of cortisol were
examined across four time po ints during attendance in a residential
sleep intervention program and at one time point after mothers and in-
fants compl eted the program and returned home (scheduled for the
first weekend night of the second week at home to accommodate com-
pletion of the sleep log and saliva sampling). At each time point, cortisol
levels were assessed at wake, initiation of infant sleep routine, and
20 min after infants transitioned to sleep. Infant TST and cortisol levels
were examined across mothers' self-reported levels of depression,
anxiety, and stress. The intervention at the participating facility provid-
ed a 5-day/4-night intervention program for mothers who reported
their infants as exhibiting significant sleep problems defined as multiple
overnight wakings, infant distress at day and night sleep settling times,
and a history of extended settling periods.
2.2. Study population
Participants were 34 mother-infant dyads (Mother M
age
= 32.59,
range 23–41 years; infant M
age
= 7.16 months, age range 4–11 months;
16 males) who were admitted to a public residential family-care facility
in an urban area in Australia. Demographic data were available from 23
of the participating mothers. Based on this data, 17 mothers reported
being born in Australia. Other reported countries of birth included
New Zealand, India, United States, South Africa, Malaysia, and the Unit-
ed Kingdom, with 1 participant from each country. 22 mothers reported
currently having a partner with partnership status either legally mar-
ried (n = 19) or defacto relationship (n = 3). One mother reported
being divorced or my marriage has dissolved. The target child was the
only child for 15 mothers and 8 mothers reported the infant to be
their second child. Mothers' education level ranged from secondary
school before Year 12 (n = 1), Year 12 (n = 2), University Certificate
(n = 6), Bachelors (n = 6), Graduate Diploma (n = 1), Masters (n =
6), and Doctorate (n = 1). Mothers' reported total family income (in
Australian dollars) from $15,000 to $30,000 (n = 2), $30,000 to
$50,000 (n = 2), $50,000 to $70,000 (n = 3), $70,000 to $100,000 (n
= 6), and $100,000+ (n = 7).
50 W. Middlemiss et al. / Early Human Development 108 (2017) 49–57
2.3. Procedures
2.3.1. Recruitment
All mothers with infants between 4 and 10 months of age referred to
the residential program were advised of the study prior to admission to
the residential center. 64 mothers were invited to participate. Of these
mothers, 54 (84%) agreed to participate in the study with their infant.
Of these 54 mothers, 20 (37%) withdrew during their participation.
Fifteen mothers withdrew because they feared cortisol collection fol-
lowing infants' transition to sleep would wake their infant; 1 withdrew
as engaging in the sleep program and study was too much pressure, 1
withdrew based on mental health concerns, and the reason for with-
drawing for 1 mother was unknown.
Upon arrival, mothers eligible to participate were provided with in-
formation regarding the research and those choosing to participate
signed an informed consent. The project had ethics approval from the
Human Research Ethics Committee Mercy Health, Melbourne, Australia,
the health facility human ethics committee, as well as the respective ac-
ademic institutions of each researcher. All participating mothers were
assured verbally and in writing that there was no penalty for choosing
not to engage in the study. Mothers were a ssured that they may
withdraw from the study at any time. Mothers who smoked, were on
prescription antidepressant medication, or steroid based anti-inflam-
matory medication were excluded from the study, as these alter salivary
cortisol. To ensure consistency of information provided to mothers, the
registered nurses on the admission shifts were the only responsible
parties for determining whether or not the dyads fi t the criteria and
alerting the researcher of the mother's interest and location.
2.3.2. Recording sleep hours
During the residential intervention program, Maternal and Child
Health nurses and qualified early childhood workers together with the
infants' mothers maintained the wake and sleep log on program Days
1, 2, and 3 of the residential intervention. Mothers recorded hours of
wake and sleep time in their homes for a 24-hour period nine days
after intervention completion. At admission and following consent to
participate in the study, mothers were asked to respectively log infant
hours of sleep across the two days immediately prior to admission.
2.3.3. Intervention
The residential program incorporates education on normative sleep
patterns, including night wakings, in an effort to move parents toward
considerin g the infant's need of emotional and physical nutrition
when transitioning to sleep. Emphasis is placed on the needs of infants
to have access to parental care during this time and the importance of
contingently responsive care to the infant cues and behaviors, both
day and night. During the period of infant settling, parents are encour-
aged to provide progressively increasing parental care, based on the
infant cues and behaviors.
This care starts with parents watching for and responding to infant
sleep signs. Parents are encouraged to develop consistent sleep prepara-
tion that includes a predictable set of events that can be replicated once
home, such as quiet time before sleep, which includes direct physical
contact with the parent including book reading and or massage. Infant
needs at the time of separation for sleep are discussed, including the
need for parental emotional availability during this period.
Parents are encouraged to listen to the infant and offer care in re-
sponse to infants' communication. This guides parents away from either
intrusive or non-contingent care. In the event infants cry, parents are
coached to respond with low leve l support care and b uild it over a
short period of time, e.g., no longer than 15 to 30 s econds. This low
level of supportive care can include quiet verbal comforting, stroking
the infant, patting the mattress, or other low level calming responses.
During this short length of time, parents have the opportunity to
watch and listen for cues, and the infant has the opportunity to self-
regulate.
Parents are advised that it is important that the infant is not left to
cry. If soothing without picking up their infant does not calm the infant,
parents are encouraged to provide increasing levels of response and at-
tention until they can soothe their infant, which includes cuddling or
feeding to comfort. When responding to t heir infants' waking over-
night, parents are encouraged to tune into the infants' communication
before intervening and are encouraged to observe for and respond to in-
fant cues and behavior. This type of attending and responding over time
provides both parent and infant predictability of contingent parental re-
sponse to infant cues. This ensures the infant is not left to cry but rather
is offered comforting when unable to calm. By encouraging the parent
to offer contingent care, tired parents experience how the cues of the in-
fant lead the care which ultimately results in calm sleep transitioning
and longer sleep hours. This cue based care ensures each individual's
communication and capacity is factored into the care planning.
This development of synchrony of parental attention and response
to infant communication in the form of cues and behavior is encouraged
and guided by the facility nursing staff. The residential center policy
promotes ‘care by parent’ whereby staff guide and support parents in
watching for and thinking about both the communication of their infant
and their responses to their infants' signals. Promotion of mothers'
capacity to look at and listen to their infants and respect infant experi-
ences is an integral component of the intervention.
2.4. Instruments and measures
2.4.1. Demographic background information
After consenting, mothers completed a demographic questionnaire;
information for 23 mothers was available for reporting at the time of
analyses. Information for the remaining participants was not completed.
2.4.2. Infant TST
The sleep log [36]
used at the facility to track sleep and wake behav-
ior
s provided the measure of infant TST prior to admission, during Days
1, 2, and 3 of the intervention, and at the ninth day after mothers and in-
fants returned home. The sleep log provides an efficient way to track
sleep and wake times and has been used in a number of trials to date
[36]. On Days 1, 2, and 3, the sleep log was maintained by the Centre
staff and mothers. Mothers completed the sleep log for the home assess-
ment following program completion. Mother reports of infant TST on the
two days prior to admission were collected retrospectively following
mothers' admission and consent to participate in the research project.
2.4.3. Edinburgh Postnatal Depression Scale (EPDS)
The EPDS is a self-rating scale originally designed to help identify
risk of postnatal depression [37]. This validated tool [38,39,40] is used
in a range of perinatal disciplines to screen for antenatal and postnatal
evidence of depressive symptoms [41]. In this study, the EPDS was com-
pleted by th e consenting mother at, or close to, adm ission . Mothers
were identified as at probable risk of depression when scores were
≥ 13 [42,43].
2.4.4. Depression, Anxiety, and Stress Scale 21 (DASS-21)
The DASS-21 [44,45,46] is a self-administered instrument measuring
the intensity of risk of depressive, anxiety and stress symptoms [46,40]
with the scoring categories relating to the intensity of the symptoms.
DASS-21 cut-off scores for severe or extremely severe levels of symp-
tomatology for depression, anxiety, or stress were ≥ 21 for depression,
≥ 15 for anxiety, and ≥ 26 for stress. DASS-21 cut-off scores for moderate
or greater levels of symptomatology for depression, anxiety, or stress
were ≥ 14 for depression, ≥ 10 for anxiety, and ≥ 19 for stress.
2.4.5. Salivary cortisol levels
Maternal and infant salivary cortisol was assessed at three time
points (wake, initiation of infant nighttime sleep routine, and 20-mi-
nutes after infants had transitioned to sleep) during each of the program
51W. Middlemiss et al. / Early Human Development 108 (2017) 49–57
days and on the ninth day after their return home. Mothers donat ed
2 ml of saliva into the appropriate pathology tube, while infant saliva
was collected via sorbette. All samples were frozen in a dedicated, mon-
itored freezer until collection and transport frozen in a laboratory sup-
plied truck to the pathology laboratory. Home samples were stored in
freezers and transported in thermo-regulated containers to assure sam-
ples remain ed frozen until reaching the laboratory. Salivary cortisol
samples were assayed using a highly-sensitive enzyme immunoassay
(Salimetrics, State College, PA). The test used 25 μlofsaliva,hada
lower limit of sensitivity of 0.007 μg/dl, and a range of sensitivity from
0.007 to 3.0 μg/dl [average intra- and inter-assay coefficients of variation
of b 10% and 15%, respectively]. Outliers were identified as individual
scores that exceeded their respective means by at least 3 standard devi-
ations. Salivary assays were completed at Salivary Laboratory, Stratech
Scientific, Inc., APAC Pty, Ltd., Sydney, Australia.
2.5. Preliminary analyses
A multiple imputation method was conducted to impute mi ssing
values for variables in the dataset. These values are assumed to be miss-
ing at random and avera ges were pooled to esti mate missing data
points. To determine the association between mothers' measures of de-
pression and other measures of well-being, correlational analyses were
computed. Mothers' DASS-21 scores were significantly positively corre-
lated with mothers' EPDS scores (r = 0.72, r = 0.61, and r = 0.62 for
DASS-21 depression, anxiety, and stress scores, respectively).
3. Results
3.1. Infant TST
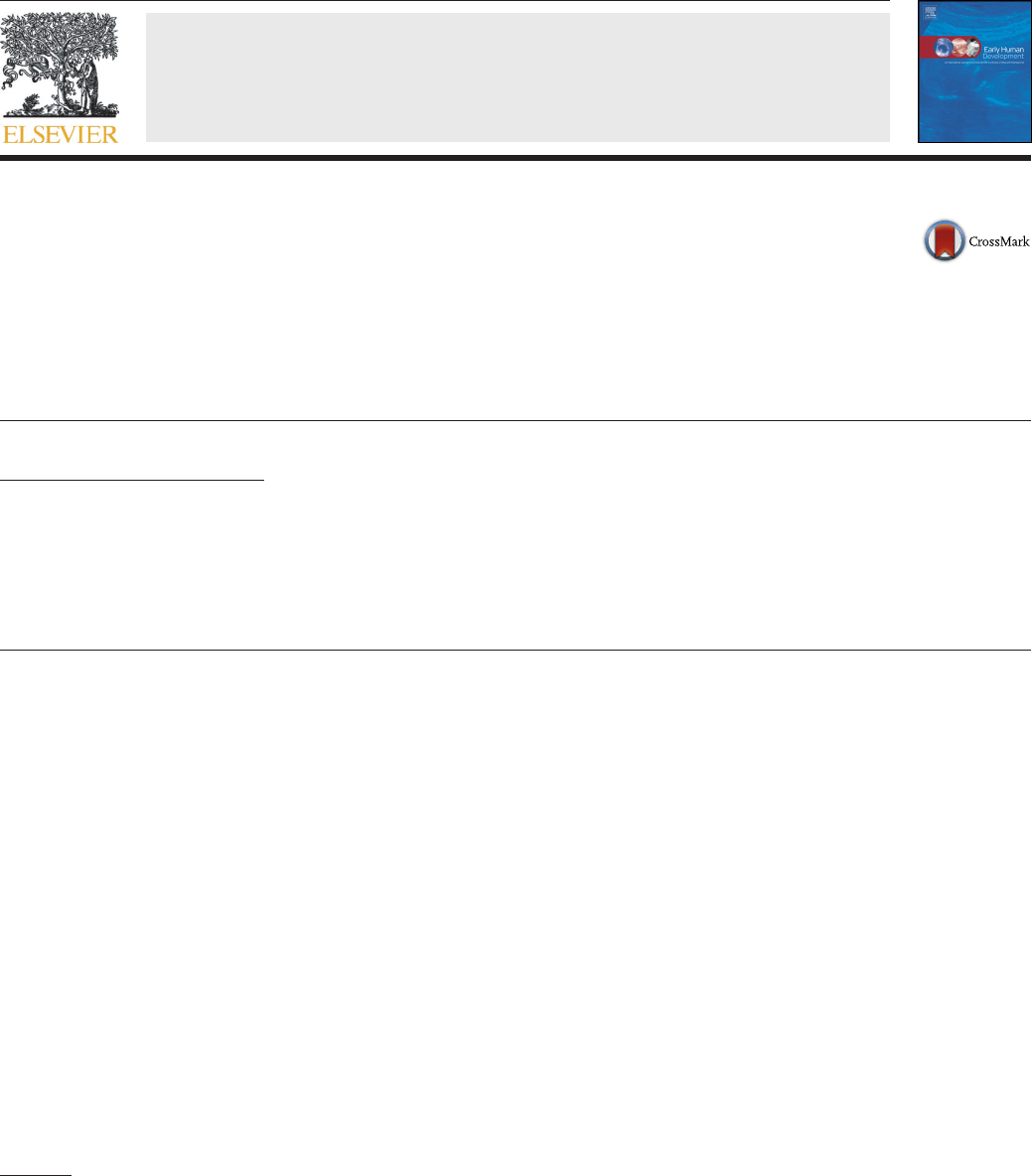
Based on assessment of TST reported in the sleep logs by mothers
(Pre-Admission and Home assessment times) and nurses (Days 1–3as-
sessment times), infant TST after return Home was significantly higher
than at Pre-Admission (t(59) = 8.96, p b 0.001; Fig. 1). During Days 1
through 3 of the residential program, infant TST significantly increased
from Day 1 to Day 2 (t(510) = 3.12, p = 0.002), Day 2 to Day 3
(t(345) = 5.97, p b 0.001), and Day 3 to Home (t(581) = 4.20, p b
0.001) (Fig. 1). Hypothesis 1.3.1 was supported.
3.2. EPDS
3.2.1. EPDS and change in infant TST
Mothers' EPDS scores ranged from 5 to 22 (M = 15.1). Change in in-
fant TST was compared between those mothers who scored at or above
the symptomatic cutoff score of 13 (n = 26, 76%) and those who scored
below 13 (n = 8). A repeated measures analysis of variance (ANOVA)
identified a significant effect of program participation on infa nt TST
both for infants whose mothers scored above (F(4,22) = 33.38, p b
0.001, η
p
2
= 0.57) and infants whose mothers scored below (F(4,4) =
19.63, p b 0.001, η
p
2
= 0.73) the cutoff score of 13. Greenhouse-Geisser
analyses were reported to adjust for a violation of sphericity. Paired-
sample t-tests computed to determine direction of effect of program
participation on infant TST from Pre-Admission to Home hours found
infant TST was significantly higher after return Home than Pre-Admis-
sion for both infants whose mothers scored above (t(46) = 7.14, p b
0.001) a nd infants whose mot hers scored below (t(91) = 5.86, p =
0.001) the cutoff score.
Paired sample t-tests were computed to examine significance of
mean difference in infant TST across the days of program participation.
For mothers scoring above the cutoff score for severe or very severe de-
pression, infant TST increased significantly from Day 1 to Day 2 (t(2863)
=2.65,p =0.01),Day2toDay3(t(2222) = 4.83, p b 0.001), and Day 3
to Home (t(338) = 3.01, p = 0.005) (Table 1). For mothers scoring
below the cutoff score for depression, infant TST increased significantly
between Day 2 to Day 3 (t(132) = 5.96, p = 0.0001) and Day 3 to Home
(t(59) = 3.19, p = 0.01) (Table 1). Hypothesis 1.3.1 was supported.
3.2.2. TST across EPDS symptomatology
For each day of participation, i.e., Pre-Admission, program Days 1–3,
and Home, infant TST was compared between infants whose mothers
scored above and infants whose mothers scored below the cutoff
score of 13. No significant differences in TST were identified on any of
the days.
3.2.3. EPDS prediction of change in TST
Mothers' EPDS score at intake did not explain variance in infant sleep
hours at Pre-Admission, program days, or Home measures based on
ANOVAs computed at each time point.
3.3. DASS-21 depression
3.3.1. Severe symptomatology for depression
Mothers' DASS-21 depression scores ranged from 4 to 24 (M = 14.2)
with 17% (n = 6) scoring at or above the symptomatic depression cutoff
score of 21 indicating severe to very severe symptomatology for depres-
sion. A repeated measures analysis of variance (ANOVA) identified a sig-
nificant effect of program participation on infant TST both for infants
whose mothe rs scored above (F(4,2) = 12.26, p =0.01,η
p
2
=0.68)
and infants whose mothers scored below (F(4,3) = 41.34, p b 0.001,
η
p
2
= 0.60) the cutoff score of 21. Greenhouse-Geisser analyses were re-
ported to adjust for a violation of sphericity. Paired-sample t-tests com-
puted to determine direction of effect of program participation on infant
TST from Pre-Admission to Home hours found infant TST was signifi-
cantly higher after return Home than Pre-Admission for both infants
whose mothers scored above (t(40) = 3.38, p = 0.002) and mothers
who scored below (t(68) = 8.26, p b 0.001) the cutoff score of 21
(Table 1).
Paired sample t-tests were computed to examine significance of
mean difference in infant TST across each of the days of program partic-
ipation. For mothers whose scores indicated severe or very severe de-
pression, infant TST significantly increased from Day 1 to Day 2 (t(5)
=4.57,p b 0.001) and Day 2 to Day 3 (t(5) = 3.08, p = 0.002). For
mothers whose scores did not indicate symptomatology, infant TST sig-
nificantly increased from Day 1 to Day 2 (t(505) = 2.63, p = 0.009), Day
2toDay3(t(301) = 5.53, p b 0.001), and Day 3 to Home (t(393) = 3.80,
p b 0.001) (Table 1; Fig. 2). Hypothesis 1.3.1 was supported.
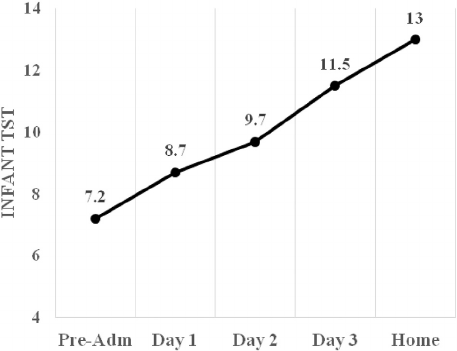
3.3.2. TST across DASS-21 depression scores
For each day of participation, i.e., Pre-Admission, program Days 1–3,
and Home, infant TST was compared between infants whose mothers
scored above and infants whose mothers scored below the cutoff
Fig. 1. Infant total sleep time (TST) per day from preadmission to home report. (n = 34).
52 W. Middlemiss et al. / Early Human Development 108 (2017) 49–57
score of 21. Based on independent-samples t-tests, infant TST was sig-
nificantly different only for infants' Home TST. Home TST was signifi-
cantly lower for infants whose mothers' scores indicated severe or
very severe symptomatology in comparison to infants whose mothers'
scores did not indicate severe or very severe symptomatology (t(160)
= 2.58, p = 0.01). Hours of sleep between infants whose mot hers
scored above or below the cutoff score of 21 were not significantly dif-
ferent at Pre-Admission or program Days 1–3.
3.3.3. Moderate symptomatology for DASS-21 depression
Analyses were completed to examine infant TST when a cutoff score
indicating moderate symptomatology was used. These analyses com-
pared effect of program participation on infant TST for infants whose
mothers scored at or above the DASS-21 cutoff score of 14 (61%, n =
21). A repeated measures ANOVA identified a significant effect of pro-
gram participation on infant TST both for infants whose mothers scored
above (F(4,3) = 32.14, p b 0.001, η
p
2
= 0.61) and infants whose mothers
scored below (F(4,4) = 19.25, p b 0.001, η
p
2
= 0.61) this cutoff point for
moderate symptomatology. Greenhouse-Geisser analyses were report-
ed to adjust for a violation of sphericity. Paired-sample t-tests computed
to determine direction of difference in TST from Pre-Admission to Home
hours found infant TST was significantly higher after return Home than
at Pre-Admission for both infants whose mothers scored above (t(73)
= 7.42, p b 0.001) and mothers who scored below (t(72) = 5.33, p b
0.001) the cutoff score.
Paired sample t-tests computed to examine significance of mean dif-
ference in infant TST across the days of program participat ion. For
mothers whose scores indicated moderate or higher symptomatology
for depression, infant TST significantly increased from Day 1 to Day 2
(t(1369) = 2.17, p = 0.03), Day 2 to Day 3 (t(1 029) = 4.14, p ≤
0.001), and Day 3 to Home (t(187) = 3.69, p b 0.001) (Table 2). For
mothers whose scores indicated moderate to no symptomatology, in-
fant TST significantly increased from Day 1 to Day 2 (t(410) = 2.25, p
=0.03)andDay2toDay3(t(232) = 4.53, p b 0.001) (Table 2).
3.4. DASS-21 anxiety
3.4.1. Severe symptomatology for anxiety
Maternal DASS-21 anxiety scores ranged from 2 to 24 (M = 13.4)
with 50% (n = 17) scoring at or above the symptomatic anxiety cutoff
score of 15 indicating severe to very severe symptomatology for anxiety.
A repeated measures ANOVA identified a significant effect of program
participation on infant TST both for infan ts whose mothers scored
above (F(4,13) = 32.22, p = 0.01, η
p
2
= 0.66) and infants whose
mothers scored below (F(4,13) = 32.23, p b 0.001, η
p
2
= 0.66) the cutoff
score of 15. Greenhouse-Geisser analyses were reported to adjust for a
violation of sphericity. Paired-sample t-tests computed to determine ef-
fect of program participation on infant TST from Pre-Admission to Home
hours found infant TST was significantly higher after return Home than
at Pre-Admission for both infants whose mothers scored above (t(62)
=6.84,p b 0.001) and mothers who scored below (t(98) = 6.07, p =
0.01) the cutoff score of 15.
Paired sample t-tests were computed to examine significance of
mean difference in infant TST across the days of program participation.
For mothers scoring above the cutoff score for severe or very severe
anxiety, infant TST significantly increased from Pre-Admission to Day
1(t(32) = 2.14, p = 0.04), Day 1 to Day 2 (t(860) = 3.40, p =
0.001), and Day 2 to Da y 3 (t(483) = 4.87, p b 0.001) (Table 1). For
mothers whose scores indicated symptomatology below the severe cut-
off score, infant TST significantly increased from Day 2 to Day 3 (t(552)
=3.74,p = 0.001) and Day 3 to Hom e (t(265) = 4.42, p = 0.001)
(Table 1). Hypothesis 1.3.1 was supported.
3.4.2. TST across DASS-21 anxiety scores
For each day of participation, i.e., Pre-Admission, program Days 1–3,
and Home, infant TST was compared between infants whose mothers
scored above and infants whose mothers scored below the cutoff
Table 1
Infant Total Sleep Time across mothers scoring above or below the EPDS and DASS-21 severe cutoff scores.
Pre-Adm Day 1 Day 2 Day 3 Home Pre-Adm–Home
All infants 7.2 (2.9) 8.7 (2.0)
⁎
9.7 (1.8)
⁎⁎
11.5 (1.9)
⁎⁎⁎
13.0 (1.8)
⁎⁎⁎
7.2–13.0
⁎⁎⁎
EPDS
Severe–very severe 7.5 (0.69) 8.8 (0.40) 9.8 (0.39)
⁎⁎
11.6 (0.40)
⁎⁎⁎
12.8 (0.40)
⁎⁎⁎
7.5–12.8
⁎⁎⁎
Not severe 6.2 (1.08) 8.2 (0.82) 9.2 (0.49)
⁎⁎⁎
11.2 (0.61)
⁎⁎⁎
13.4 (0.59)
⁎⁎
6.2–13.4
a
DASS-21 depression
Severe–very severe 5.8 (1.50) 8.3 (0.61) 9.2 (0.53)
⁎⁎⁎
10.3 (0.79)
⁎⁎
11.3 (0.99) 5.8–11.3
⁎⁎
Not severe 7.5 (0.62) 8.8 (0.42) 9.8 (0.38)
⁎⁎
11.7 (0.35)
⁎⁎⁎
13.3 (0.32)
⁎⁎⁎
7.4–13.3
⁎⁎⁎
DASS-21 anxiety
Severe–very severe 6.7 (0.88) 8.6 (0.42)
⁎
10.0 (0.46)
⁎⁎⁎
11.9 (0.50)
⁎⁎⁎
12.9 (0.52) 6.8–12.9
⁎⁎⁎
Not severe 7.6 (0.76) 8.8 (0.60) 9.3 (0.45) 11.1 (0.43)
⁎⁎⁎
13.0 (0.43)
⁎⁎⁎
7.6–13.0
⁎⁎⁎
DASS-21 anxiety
Severe–very severe 6.9 (1.60) 8.9 (0.66) 9.9 (0.65)
⁎⁎⁎
10.9 (0.83)
⁎
11.9 (0.85) 0.9–11.9
⁎⁎
Not severe 7.3 (0.60) 8.6 (0.43) 9.6 (0.34)
⁎
11.7 (0.36)
⁎⁎⁎
13.3 (0.35)
⁎⁎⁎
7.2 (13.3)
⁎⁎⁎
Note. EPDS Severe symptomatology (≥13); DASS-21 Depression Severe symptomatology (≥ 21); DASS-21 Anxiety Severe symptomatology (≥15); DASS-21 Stress Severe symptomatology
(≥ 26).
a
= approached significance.
⁎
p ≤ .05.
⁎⁎
p ≤ .01.
⁎⁎⁎
p ≤ .001.
Fig. 2. Hours of infant sleep for infants whose mothers' DASS-21 scores indicated presence
of severe and extremely severe symptomatology for depression and mothers whose
scores did not indicate this level of symptomatology. Infants total sleep time (TST) was
significantly different at the Home sleep.
53W. Middlemiss et al. / Early Human Development 108 (2017) 49–57
score of 15. No significant differences in TST were identified based on
independent-samples t-tests.
3.4.3. Moderate symptomatology for anxiety
Analyses were completed to examine infant TST when a cutoff score
indicating moderate symptomatology was used. These analyses com-
pared effect of program participation on infant TST for infants whose
mothers (71%, n = 24) scored at or above the cutoff score of 10. A re-
peated measures ANOVA identified a significant effect of program par-
ticipation on infant TST both for infants whose mothers scored above
(F(4,2) = 38.70, p b 0.001, η
p
2
= 0.63) and infants whose mothers scored
below (F(4,6) = 12.20, p b 0.001, η
p
2
= 0.57) this cutoff point for mod-
erate symptomatology. Greenhouse-Geisser analyses were reported to
adjust for a violation of sphericity. Paired-sample t-tests computed to
determine direction of difference in TST from Pre-Admission to Home
hours found infant TST was significantly higher after return Home
than infant TST at Pre-Admission for both infants whose mothers scored
above (t(53) = 8.02, p b 0.001) and mothers who scored below (t(286)
=4.36,p b 0.001) the cutoff score of 10 (Table 2).
Paired sample t-tests were computed to examine significance of
mean difference in infant TST across each of the days of program partic-
ipation. For mothers scoring at or above the cutoff score for moderate
symptomatology for anxiety, infant TST significantl y increased from
Pre-Admission to Day 1 (t(46) = 2.08, p = 0.04), Day 1 to Day 2
(t(1690) = 3.32, p = 0.001), Day 2 to Day 3 (t(2075) = 4.65, p b
0.001), and Day 3 to Home (t(250) = 3.13, p =002)(Table 2). For
mothers scored below the cutoff score, infant TST increased from Day
2toDay3(t(58) = 4.13, p b 0.0001) and Day 3 to Home (t(95) =
2.78, p = 0.007) (Table 2). Hypothesis 1.3.2 regarding infant TST and
mothers' DASS-21 anxiety scores was supported.
3.5. DASS-21 stress
3.5.1. Severe symptomatology for stress
Mothers' DASS-21 stress scores ranged from 1 to 33 (M = 19.4) with
24% (n = 8) scoring at or above the DASS-21 stress cutoff score of 26,
indicating severe to very severe symptomatology for stress. A repeated
measures ANOVA identified a significant effect of program participation
on infant TST both for infants whose mothers scored above (F(4,4) =
9.73,pb 0.001, η
p
2
= 0. 56) and infants whose mothers scored below
(F(4,22) = 43.09, p b 0.001, η
p
2
= 0.63) the cutoff score of 26. Green-
house-Geisser analyses were reported to adjust for a violation of sphe-
ricity. Paired-sample t-tests computed to determine direction of effect
of program participation on infant TST from Pre-Admission to Home
hours found infant TST was significantly highe r after return Home
than Pre-Admission for both infants whose mothers scored above
(t(32) = 3.27, p b 0.001) and infants whose mothers scored below
(t(73) = 8.50, p b 0.001) the cutoff score of 26 (Table 1).
Paired sample t-tests were computed to examine significance of
mean difference in infant TST across each of the days of program partic-
ipation. For mothers whose scores indicated severe or very severe
stress, infant TST increased from Day 1 to Day 2 (t(7) = 6.11, p b
0.001) and Day 2 to Day 3 (t(7) = 2.38, p = 0.02) (Table 1). For mothers
whose scores did not indicate symptomatology, infant TST increased be-
tweenDay1toDay2(t(506) = 2.40, p = 0.02), Day 2 to Day 3 (t(249)
=5.71,p b 0.001), and Day 3 to Home (t(219) = 3.78, p b 0.001) (Table
1). Hypothesis 1.3.1 was supported.
3.5.2. TST across DASS-21 stress scores
For each day of participation, i.e., Pre-Admission, program Days 1–3,
and Home, infant TST was compared between infants whose mothers
scored above and infants whose mothers scored below the cutoff
score of 26. Based on independent-samples t-tests, infant TST was not
significantly different between these groups of infants on any of these
program days.
3.5.3. Moderate symptomatology for stress
Analyses were completed to examine infant TST when a cutoff score
indicating moderate symptomatology was used. These analyses com-
pared effect of program participation on infant TST for infants whose
mothers (56%, n = 19) scored at or above the cutoff score of 19 indicat-
ing moderate to very severe symptomatology for stress. A rep eated
measures ANOVA identified a significant effect of program participation
on infant TST both for infants whose mothers scored above (F(4,15) =
31.18, p = 0.01, η
p
2
= 0.64) and infants whose mothers scored below
(F(4,11) = 19.93, p b 0.001, η
p
2
= 0.59) this cutoff point for moderate
symptomatology. Greenhouse-Geisser analyses were reported to adjust
for a violation of sphericity. Paired-sample t-tests computed to
Table 2
Infant Total Sleep Time across mothers scoring above or below the DASS-2.
Pre-Adm Day 1 Day 2 Day 3 Home Pre-Adm – Home
DASS21 Depression
Moderate or above 7.5 (0.70) 8.9 (0.45) 9.8 (0.40)
⁎
11.3 (0.40)
⁎⁎⁎
13.1 (0.48)
⁎⁎⁎
7.5–13.1
⁎⁎⁎
Below moderate cutoff 6.6 (0.98) 8.2 (0.61) 9.5 (0.56)
⁎
11.7 (0.60)
⁎⁎⁎
12.8 (0.46) 6.6–12.8
DASS21 anxiety
Moderate to very severe 7.1 (0.71) 8.7 (0.45)
⁎
9.9 (0.39)
⁎⁎
11.7 (0.43)
⁎⁎⁎
13.2 (0.44)
⁎⁎
7.1–13.2
⁎⁎⁎
Below Moderate cutoff 7.4 (1.03) 8.6 (0.61) 9.1 (0.58) 10.9 (0.44)
⁎⁎⁎
12.5 (0.44)
⁎⁎
7.4–12.5
⁎⁎
DASS21 stress
Moderate to very severe 7.5 (0.76) 8.9 (0.41) 9.9 (0.44)
⁎⁎⁎
11.5 (0.44)
⁎⁎⁎
12.5 (0.44)
⁎⁎
7.5–12.9
⁎⁎
Below moderate cutoff 6.8 (0.86) 8.4 (0.65) 9.4 (0.49) 11.5 (0.53)
⁎⁎⁎
13.0 (0.48)
⁎⁎
6.8–13.0
⁎⁎⁎
Moderate cutoff scores.
Note. DASS-21 Depression Moderate symptomatology (≥14); DASS-21 Anxiety Moderate symptomatology (≥10); DASS-21 Stress Moderate symptomatology (≥19).
⁎
p ≤ 0.05.
⁎⁎
p ≤ 0.01.
⁎⁎⁎
p ≤ 0.001.
Table 3
Mother DASS-21 depression, anxiety, and stress scores at admission as related to infant
TST following program completion.
DASS-21 B SE Beta tp
Anxiety −0.017 0.039 −0.486 2.473 0.02
Depression −0.052 0.033 0.513 −2.018 0.05
Stress 0.083 0.029 0.117 0.545 0.59
Note. n = 34.
Table 4
Mothers' cortisol levels at each collection time across intervention and home samples.⁎
Day 1 Day 2 Day 3 Home
Wake − 1.26 (0.55) − 1.04 (0.62) − 1.56 (0.69)
Presleep − 2.51 (0.53)
Day4⁎
− 2.64 (0.63) − 2.52 (0.50) − 2.88 (0.68)
Day1⁎
Postsleep −2.86 (0.53) − 2.78 (0.92) − 2.89 (0.61) − 2.87 (0.69)
Note. n=34.
⁎
p b 0.05.
Day⁎
indicates significant change between days indicated.
54 W. Middlemiss et al. / Early Human Development 108 (2017) 49–57

determine direction of effect in TST from Pre-Admission to Home hours
found infant TST was significantly higher after return Home than at Pre-
Admission for both infants whose mothers scored above (t(68) = 6.90,
p b 0.001) and those who scored below (t(108) = 6.10, p b 0.001) the
cutoff score of 19 (Table 2).
Paired sample t-tests were computed to examine significance of
mean difference in infant TST across each of the days of program partic-
ipation. For mothers who scored above the cutoff score, infant TST in-
creased from Day 1 to Day 2 (t(352) = 3.42, p = 0.001), Day 2 to Day
3(t(437) = 4.84, p b 0.001), and Day 3 to Home (t(312) = 3.08, p =
0.002) (Table 2). For mothers who scored below the cutoff, infant TST
increased from Day 2 to Day 3 (t(553) = 3.86, p b 0.001) and Day 3 to
Home (t(287) = 2.69, p = 0.008) (Table 2). Hypothesis 1.3.2 regarding
infants' TST and mothers' DASS-21 stress scores was supported.
3.6. DASS-21 scores and infant TST
Linear regression models were computed to determine whether
mothers' DASS-21 scores at intake predicted infants' hours of sleep re-
ported at preadmission; intervention Days 1, 2, or 3; or at the Home as-
sessment. Based on these analyses, mothers' DASS-21 depression and
anxiety scores predicted infants' total sleep time at Day 3 (Table 3).
3.7. Mother and infant cortisol levels
Paired samples t-tes ts we re computed to examine changes in
mothers' and infants' cortisol levels at wake, at the beginning of the
nighttime sleep routine, and 20-minutes after infants transitioned to
sleep (Tables 4 and 5; Fig. 3). The hypothesis that cortisol levels would
decrease from the beginning of the intervention through salivary sam-
ples at Home collection time was supported for mothers at presleep.
Mothers' cortisol le vels on Da y 1 presleep we re significantly higher
than at the presleep home measure (t =2.18,p = 0.038). No significant
differences were fou nd between moth ers' cortisol levels at wake or
postsleep samples.
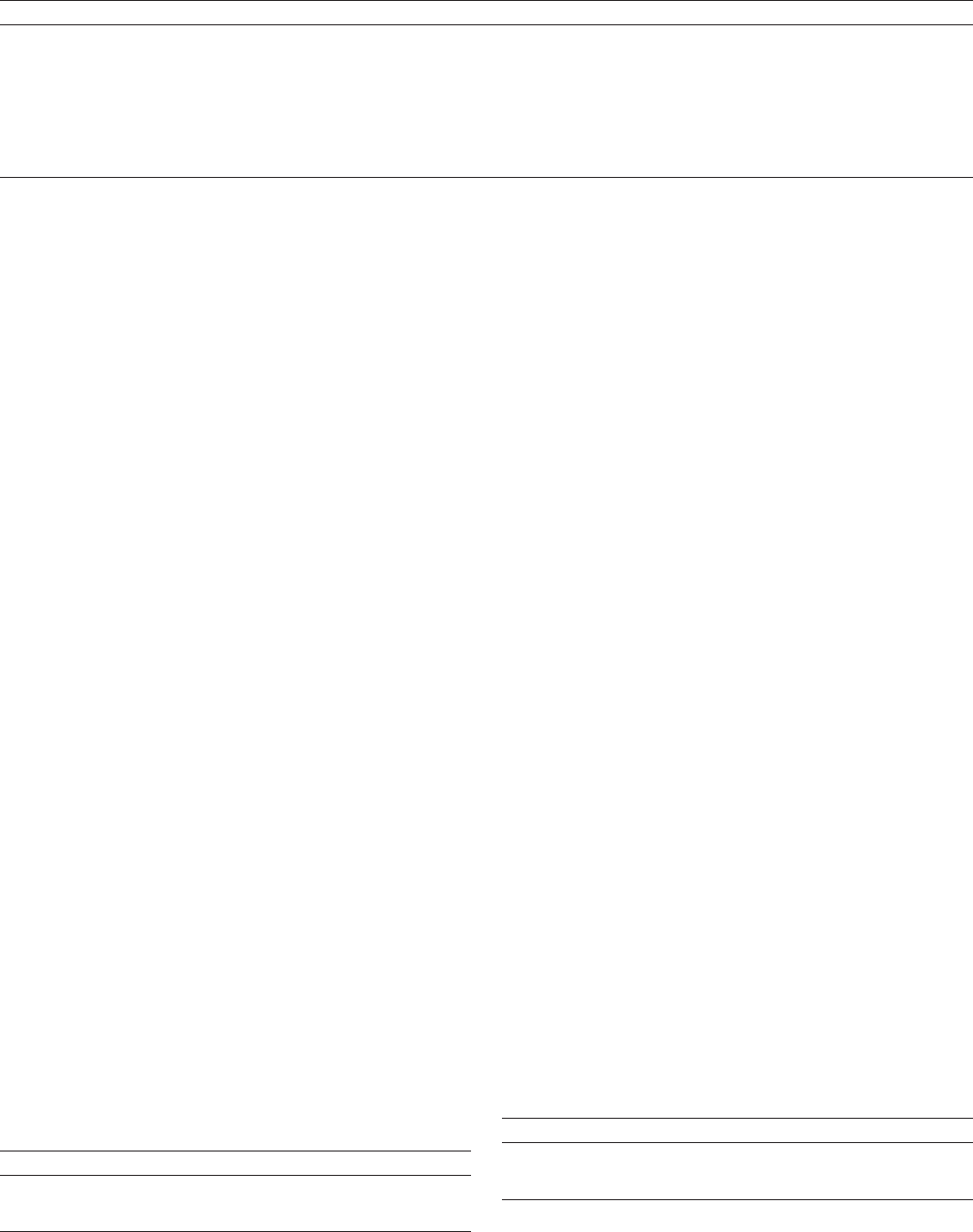
Based on paired samples t-tests, infants' cortisol levels at the pre-
sleep collection were significantly higher at the Day 2 in comparison
to the Home measure (t =2.01,p = 0.05). Infants' cortisol levels at
the postsleep collection were significantly higher at the Day 3 in com-
parison to the Home m easure (t =2
.39,p = 0.03). Infants' cortisol
levels were significantly lower on Day 1 postsleep in relation to Day 2
postsleep levels (t =2.72,p = 0.01).
4. Discussion
Teaching parents to understand and respond to infant cues, through
the day and at transitions to sleep, was associated with an increase in
infants' TST in mothers identifying their infants' sleep schedules as
problematic prior to their participation in a response based sleep inter-
vention. The changes in infant sleep time across mothers experiencing
depression, anxiety, and stress further support response-based inter-
vention as a viable approach to supporting parents in helping their in-
fants sleep. Of particular importance in regard to infant sleep research
and practice is the finding that infants' sleep time can be increased with-
out engaging in behavioral extinction programs necessitating parental
nonresponse to infant cues. This research provides, to the knowledge
of the authors, the first empirically supported examination of re-
sponse-based sleeping interventions to increase infant sleep. In addition
to longer sleep time, a primary goal of many sleep interventions, the in-
tervention focuses on respo nsiveness. The importance of reading in-
fants' cues in a synchronous manner is clearly supported throughout
developmental literature. Thus, the benefit of this approach in compar-
ison to interventio ns that necessitate parental nonresponse to infant
cues, is theoretically important [19,20,22]. These findings provide infor-
mation important for both clinicians and parents.
In relation to parents, research continues to identify behaviorally
based, parent-absent sleep interventions to be difficult for parents
[13]. As the fundamental need for infants is responsiveness, even during
the transition to sleep time, we aim to provide parents a means of
responding to infants at sleep settling and waking times without nega-
tively impacting infant sleep patterns and stress indicators. This educa-
tional intervention involves providing parents with an approach that
incorporates their instincts to comfort distressed infants [47].
The potential benefit of focusing on infant cues rather than parental
absence when infants transition to sleep is twofold. First, this approach
provides parents with an approach to changing infant sleep patterns
without the necessity of limiting responsiveness or being absent when
infants transition to sleep. Thus, this approach can reduce the need for
behavioral interventions requiring parental absence, resulting in a
greater parent infant synchrony. Second, by focusing on recognition of
infant cues, this intervention supports parents across settings. Parents
become aware of infant cues regarding not only sleepiness but also hun-
ger, distress, or other circumstances. This is likely to have additional
benefits such as potentially impacting on parent-child interactions and
attachment into the future.
Equally important to these two outcomes, this approach to helping
parents adjust infant sleep patterns offers the infant an experience of
parental comfort during the transition to sleep thro ugh the parent
responding to the infant cues and behaviors. Research contin ues to
identify behaviorally based, parent-absent sleep interventions to be dif-
ficult for parents [13] and emotional availability as important to both
mothers' and infants' sleep quality [33]. Given the nature of behavioral
intervention, particularly the absolute importance of consistency, par-
ents' difficulty with non-responding can have a ne gative impact on
the infant sleep patterns and emotional wellbeing [12].
Patterns of increase in TST for infants acro ss levels of mothers'
depression and anxiety symptomatology are interesting to examine. In
relation to depression, mothers experiencing depressive symptoms
are less likely than other mothers to engage with their infants—whether
Table 5
Infants' cortisol levels at each collection time across intervention and home samples.
Day 1 Day 2 Day 3 Home
Wake − 1.15 − 1.16 − 1.43
Presleep − 2.40 − 2.19 − 2.35 − 2.30
Postsleep − 2.44
Day2⁎
− 1.68
Day1⁎,Day4⁎⁎
− 1.95
Day4⁎
− 2.83
Day2⁎⁎, Day3 ⁎
Note. n = 34.
⁎
p b 0.05.
Day⁎
indicates significant change between days indicated.
-3.50
-3.00
-2.50
-2.00
-1.50
-1.00
-0.50
Wake PreSleep PostSleep
Day 2
Day 3
Home
Cortisol Levels µg/dL
Fig. 3. Infant cortisol levels reported from wake, presleep, through postsleep for each
program da y. Note Day 1 is n ot shown as there wa s no wake cortisol sample for
mothers and infants because Day 1 was an arrival day.
55W. Middlemiss et al. / Early Human Development 108 (2017) 49–57
in response to their cues or synchrony of social interacti on [48].
Reflecting the difficulty infants experience in engaging moth ers
experiencing depression, infants will often disengage from expectation
for social interaction or synchronous response, noted as withdrawal
[49]. In regard to infant sleep patterns, mothers who are exhibiting de-
pression often have infants who sleep longer hours, perhaps associated
with the lack of response from the mother [50]. Although infants whose
mothers' DASS-21 scores indicate severe to very severe symptomatolo-
gy have lower TSTs than other infants, the changes in TST across the pro-
gram indicate some differences in these changes across program days.
This is evident in that the only signific ant difference between infant
TST within a program day is the Home measure of TST for these two
groups of infants. At the Home measure of TST, infants whose mothers
score above the cutoff for s ymptomatology sleep si gnificantly fewer
hours than infants whose mothers score below the cutoff (Fig. 3).
Changes in TST for infants of mothers with anxiety show a similar re-
lation. Researchers have identified maternal anxiety as associated with
fewer hours of TST for infants [51].Thisassociationreflects the greater
likelihood that mothers experiencing anxiety will wake infants while
checking on them while they sleep or responding to modest movement
of the infant during transitions across sleep states [52]. Changes in the
TST of the infants whose mothers were anxious were greater at the ini-
tiation of the program than of the infants whose mothers' scores were
not indicative of anxiety. However, the changes in TST were lower at
the end of the program with both groups of infants exhibiting similar
TST at program completion (Table 1).
Overall, this research provides evidence to support changes in infant
sleep patterns based on building parents' awareness of the importance
of responding to infant cues and behaviors. Education-based interven-
tions encouraging the parent to be guided by the behavior of the infant,
in order for timely care to be provided, requires the understanding that
each parent-child dyad will have a unique experience at sleep time. This
outcome was supported in the present research both regarding infants'
TST during the program and at return home. With this outcome, parents
are encouraged to of fer infants care during the transition to sleep
through the parent responding to infant cues and communication.
4.1. Limitations
A foreseeable li mitatio n of the project design is the small sample
size. This study is limited to presenting a first effort to study a re-
sponse-based sleep intervention. The limited demographic information
available to help delineate potential differences in changes in TST based
on birth status, i.e., premature or full-term; breast or formula fed; single
or multiples birth is a limitation in regard to generalizing the study
results.
Whether mothers had a previous mental health diagnosis was not
included as part of the inclusion/exclusion criteria, nor as a potential
contributor to quality of infant sleep, unrelated to those identified dur-
ing the program. Future research examining pre-natal factors associated
with infant sleep quality, inclusive of mothers' mental health prior to
and during pregnancy will be helpful in addressing these considerations.
Direct recruitment of participants at th e time of admission to the
sleep project did not provide for a randomly assigned group of partici-
pants. The study did not include a comparison group of mothers who
declined participation, mothers who were currently prescribed anti-de-
pressant medication, or mothers with infants who were not identified
as having sleep problems. The nature of recruitment and research de-
sign in follow-up studies will address these issues of design.
Conflict of interest
One author (HS) held a s upervisory position at the Family Centre
where the research was conducted. During the project period, HS
had minimal contact with families during their participation in the
program.
Notes or acknowledgements
There are a number of contributors without whom this work would
not have been achieved. First and foremost, we thank the participants
who agreed to contribute to research even though they were attending
a parenting program due to other challenges. Their willingness to un-
dertake additional research-related commitments was very generous
and greatly appreciated. We thank the staff and management at the par-
ticipating Melbourne-based Family Centre who embraced the research
while also continuing to support families throughout the residen tial
pr
ogram. To the many research assistants and to those who supported
funding distribution, we extend our thanks. We extend our thanks to
Mercy Health, as well, for the support of this project.
References
[1] P.L.B.J. Lucassen, W.J.J. Assendelft, J.T.M. van Eijk, J.W. Gubbels, A.C. Douwes, W.J. Van
Geldrop, Systematic review of the occurrence of infantile colic in the community,
Arch. Dis. Child. 84 (2001) 398–403.
[2] L.M. Olson, M. Inkelas, N. Halfon, M.A. Schuster, K.G. O'Connor, R. Mistry, Overview
of the content of health supervision for young children: reports from parents and
paediatricians, Pediatrics 113 (2004) 1907–1916.
[3] W. Middlemiss, C.C. Barber, R. Yaure, Rockabye baby, the big picture: an international
survey on parenting practices around the world, Poster presented at the World Associ-
ationofInfantMentalHealthWorldCongress, Prague, Czech Republic, May 2016.
[4] A. Sadeh, L. Tikotzky, A. Scher, Parenting and infant sleep, Sleep Med. Rev. 14 (2010)
89–96.
[5] R. Stremler, E. Hodnett, K. Lee, A behavioral-educational intervention to promote
maternal and infant sleep: a pilot randomized, controlled trial, Sleep 29 (2006)
1609–1615.
[6] J. Mindell, A. Sadeh, B. Wiegand, T.H. How, D.Y.T. Goh, Cross-cultural differences in
infant and toddler sleep, Sleep Med. 11 (2010) 274–280.
[7] A.M. Price, J.E. Brown, M. Bittman, M. Wake, J. Quach, H. Hiscock, Children's sleep
patterns from 0 to 9 years: Australian population longitudinal study, Arch. Dis.
Child. 99 (2014) 119–125.
[8] A. Sadeh, J. Mindell, K. Luedtke, B. Wiegand, Sleep and sleep ecology in the first three
years, J. Sleep Res. 18 (2009) 60–73.
[9] R.E. Dahl, M. El-Sheikh, Considering sleep in a family context, J. Fam. Psychol. 21
(2007) 1–3, http://dx.doi.org/10.1037/0893-3200.21.1.1.
[10] C.L. Dennis, L. Ross, Relationships among infant sleep patterns, maternal fatigue, and
development of depressive symptomatology, Birth 32 (2005) 187–193.
[11] K.H. Karraker, M. Young, Night waking in 6-month-old infants and maternal depres-
sive symptoms, J. Appl. Dev. Psychol. 28 (2007) 493–498.
[12] W. Middlemiss, R. Yaure, E. Huey, Translating research-based knowledge about in-
fant sleep into practice, J. Am. Acad. Nurse Pract. 27 (2 015) 328–337, http://dx.
doi.org/10.1002/2327-6924.12159.
[13] T.I. Morgenthaler, J. Owens, C. Alessi, B. Boehlecke, T.M. Brown, J. Coleman, ... T.J.
Swick, Practice parameters for behavioral treatment of bedtime pr oblems and
night wakings in infants and young children, Sleep 29 (2006) 1277–1281.
[14] A.M. Price, M. Wake, O.C. Ukoumunne, H. Hiscock, Five-year follow-up of harms and
benefits of behavioral infant sleep intervention: randomized trial, Pediatrics 130
(2012) 643–651.
[15] L. Loutzenhiser, J. Hoffman, J. Beatch, Parental perceptions of the effectiveness of
graduated extinction in reducing infant night-wakings, J. Reprod. Infant Psychol.
32 (2014) 282–291.
[16] N.L. McElwain, C. Booth-LaF orce, Maternal sensitivity to infan t distress and
nondistress as predictors of infant-mother attachment security, J. Fam. Psychol. 20
(2006) 247–255.
[17] R. Feldman, Parent–infant synchrony biologica l foundations and developmental
outcomes, Curr. Dir. Psychol. Sci. 16 (2007) 340–
345.
[18] D.W.
Haley, K. Stansbury, Infant stress and parent responsiveness: regulation of
physiology and behavior during still-face and reunion, Child Dev. 74 (2003)
1534–1546.
[19] S.H. Landry, K.E. Smith, P.R. Swank, Responsive parenting: establishing early founda-
tions for social, communication, and independent problem-solving skills, Dev.
Psychol. 42 (2006) 627.
[20] E.M. Leerkes, A.N. Blankson, M. O’Brien, Differential effects of maternal sensitivity to
infant distress and nondistress on social-emotional functioning, Child Dev. 80
(2009) 762–775.
[21] C. Trevarthen, K.J. Aitken, Infant intersubjectivity: research, theory, and clinical ap-
plications, J. Child Psychol. Psychiatry 42 (2001) 3–48.
[22] A. Mao, M.M. Burnham, B.L. Goodlin-Jones, E.E. Gaylor, T.F. Anders, A comparison of
the sleep-wake patterns of cosleeping and solitary-sleeping infants, Child Psychiatry
Hum. Dev. 3 (2004) 95–105.
[23] D. Narvaez, Unethical and unscientific conclusions ignore how infants are harmed.
eResponse, Pediatrics. Available from http://pediatrics.aappublications.org/con-
tent/130/4/643/ reply
[24] D. Baumrind, Authoritative parenting revisited: history and current status, in: R.E.
Larzelere, A.S. Morris, A.W. Harris, R.E. Larzelere, A.S. Morris, A.W. Harrist (Eds.), Au-
thoritative Parenting: Synthesizing Nurturance and Discipline for Optimal Child De-
velopment, American Psychological Association, Washington D.C. 2013, pp. 11–34.
56 W. Middlemiss et al. / Early Human Development 108 (2017) 49–57
[25] W. Middlemiss, D.A. Granger, W.A. Goldberg, L.A. Nathans, Asynchrony of mother-
infant hypothalamic-pituitary-adrenal axis activity following extinction of infant
crying responses i nduced during the transition to sleep, Early Hum. Dev. 88
(2012) 227–232, http://dx.doi.org/10.1016/j.earlhumdev.2011.08.010.
[26] P.J. Barrasso-Catanzaro, Eslinger, neurobiological bases of executive function and so-
cial -emotional development: typical and atypical brain changes, Fam. Relat. 65
(2016) 108–119.
[27] S.D. Calkins, A. Hill, Caregiver influences on emerging emotion regulation: biological
and environmental transactions in early development, in: J. Gross (Ed.), Handbook
of Emotion Regulation, Guilford, New York 2007, pp. 229–248.
[28] T. Ha, D.A. Granger, Family relations, stress, and vulnerability: biobehavioral impli-
cations for prevention and practice, Fam. Relat. 65 (2016) 9–23.
[29] Z. Biringen, Emotional availability: conceptualization and research findings, Am. J.
Orthop. 70 (2000) 104–114, http://dx.doi.org/10.1037/h0087711.
[30] C.A. Evans, C.L. Porter, The emergence of mother–infant co-regulation during the
first year: links to infants' developmental status and attachment, Infant Behav.
Dev. 32 (2009) 147–158.
[31] L. Porter, All night long: understanding the world of infant sleep, Breastfeed. Rev. 15
(2007) 11–15.
[32] M.S. Tollenar, R. Beijers, J. Jansen, J.M.A. Riksen-Walraven, C. de Weerth, Solitary
sleeping in young infants is associated with heightened cortisol reactivity to a bath-
ing session but not to a vaccination, Psychoneuroendocrino. 37 (2012) 167–177,
http://dx.doi.org/10.1016/j.psyneuen.2011.03.
[33] D.M. Teti, B.R. Kim, G. Mayer, M. Countermine, Maternal emotional availability at
bedtime predicts infant sleep quality, J. Fam. Psychol. 24 (2010) 307–315, http://
dx.doi.org/10.1037/a0019306.
[34] L.E. Ross, B.J. Murray, M. Steiner, Sleep and perinatal mood disorders: a critical re-
view, J. Psychiatry Neurosci. 30 (2005) 247–256.
[35] L.J. Meltzer, J.A. Min dell, Relationshi p between ch ild sleep disturbances and ma-
ternal sleep, mood, and parenting stress: a pilot study, J. Fam. Psychol. 21 (2007)
67.
[36] A. Sadeh, Assessment of intervention for infant night waking: parental reports and
activity-based home monitoring, J. Consult. Clin. Psychol. 62 (1994) 63–68.
[37] J.L. Cox, J.M. Holden, R. Sagovsky, Detection of postnatal depression. Development of
the 10-item Edinburgh Postnatal D epression Scale, Brit. J. Psy chiat. 150 (1987)
782–786.
[38] J.L. Cox, G. Chapman, D. Murray, P. Jones, Validation of the Edinburgh Postnatal De-
pression Scale (EPDS) in non-postnatal women, J. Affect. Disord. 39 (1996) 185–189.
[39] M. Eberhard-Gran, A. Eskild, K. Tambs, S. Opjordsmoen, S. Ove Samuelsen, Review of
validation studies of the Edinburgh Postnatal Depression Scale, Acta Psychiatr.
Scand. 104 (2001) 243–249.
[40] F. Ng, T. Trauer, S. Dodd, T. Callaly, S. Campbell, M. Berk, The validity of the 21-item
version of the Depression Anxiety Stress Scales as a routine clinical outcome mea-
sure, Acta Neuropsychiatr. 19 (2007) 304–310.
[41] M.E. Areias, R. Kumar, H. Barros, E. Figueiredo, Comparative incidence of depression
in women and men, during pregnancy and after childbirth. Validation of the Edin-
bu
rgh Postnatal Depression Scale in Portuguese mothers, Brit. J. Psychiat. 169
(1996) 30–35.
[42] P. Boyce, J. Stubbs, A. Todd, The Edinburgh Postnatal Depression Scale: validation for
an Australian sample, Aust. Nz. J. Psychiat. 27 (1993) 472–476.
[43] J. Gibson, K. McKenzie-McHarg, J. Shakespeare, J. Price, R. Gray, A systematic review
of studies validating the Edinburgh Postnatal Depression Scale in antepartum and
postpartum women, Acta Psychiatr. Scand. 119 (2009) 350–364.
[44] M.M. Antony, P.J. Bieling, B.J. Cox, M.W. Enns, R.P. Swinson, Psychometric properties
of the 42 item and 21 item versions of the depression anxiety stress scales in clinical
groups and a community sample, Psychol. Assess. 10 (1998) 176–181.
[45] J.R. Crawford, J.D. Henry, The Depression Anxiety Stress Scales (DASS): normative
data and latent structure in a large non-clinical sample, Brit. J. Clin. Psychol. 42
(2003) 111–131.
[46] S.H. Lovibond, P.F. Lovibond, Manual for the Depression Anxiety Stress Scales, sec-
ond ed. Psychology Foundation, Sydney, 1995.
[47] P.M. Miller, M.L. Commons, The benefits of attachment parenting for infants and
children: a behavioral d evelopmental view, Behavioral Dev. Bulletin 16 (2010)
1–14, http://dx.doi.org/10.1037/h0100514.
[48] E. Tronick, C. Reck, Infants of depressed mothers, Harvard Rev. Psychiat. 17 (2009)
147–156.
[49] T. Field, B. Healy, S. Goldstein, S. Perry, D. Bendell, S. Schanberg, E.A. Zimmerman, C.
Kuhn, Infants of depressed mothers show “depressed” behavior even with nonde-
pressed adults, Child Dev. 59 (1988) 1569–1579.
[50] N.A. Jones, T. Field, N.A. Fox, B. Lundy, M. Davalos, EEG activation in 1-month-old in-
fants of depressed mothers, Dev. Psychopathol. 9 (1997) 491–505.
[51] J.L. Gress-Smith, L.J. Luecken, K. Lemery-Chalfant, R. Howe, Postpartum depression
prevalence and impact on infant health, weight, and sleep in low-income and ethnic
minority women and infants, Matern. Child Health J. 16 (2012) 887–893.
[52] A. Scher, Maternal separation anxiety as a regulator of infants' sleep, J. Child Psychol.
Psychiatry 49 (2008) 618–625.
57W. Middlemiss et al. / Early Human Development 108 (2017) 49–57
